Diabetes and the eye
Diabetes is a chronic metabolic disorder which results in the deficiency in production, secretion or utilisation of insulin in the body. This causes intolerance to carbohydrates and can lead to hyperglycaemia. Diabetes Mellitus can be classified into two types:
- Type 1 Diabetes (Insulin-dependent Diabetes Mellitus or Juvenile Onset Diabetes). This is characterised by a deficient production of insulin by the b-cells in the pancreas.
- Type 2 Diabetes (Non-insulin dependent Diabetes Mellitus or Adult-Onset Diabetes). This is when insulin may be produced but the body is ineffective in utilising it due to insulin resistance. This results in high levels of glucose in the blood. Type 2 diabetes is much more common and comprises 90% of people with diabetes worldwide.
The WHO estimates that there are 220 million people worldwide living with diabetes, and that by 2030 this figure will increase to 366. Diabetes is also the most common cause of blindness due to the ocular effects of the disorder.
Diabetic retinopathy is a microvascular complication associated with both Type 1 and Type 2 Diabetes. Its presence is mainly related to the duration of the disease than its severity. Nearly all type 1 diabetics and 77% of type 2 diabetics develop a form of retinopathy after 15 years from diagnosis. However, this incidence can be lowered by better control of blood sugar levels. In Diabetes there are a variety of haematologic abnormalities, such as increased erythrocyte aggregation, decreased red blood cell deformability, increased platelet aggragation and adhesion. These abnormalities can cause endothelial damage, slowing of the circulation and capillary closure, leading to retinal ischaemia which contributes to diabetic retinopathy. The retinal blood vessels also become more permeable resulting in transudation of serum substances which cause retinal thickening and macular oedema.
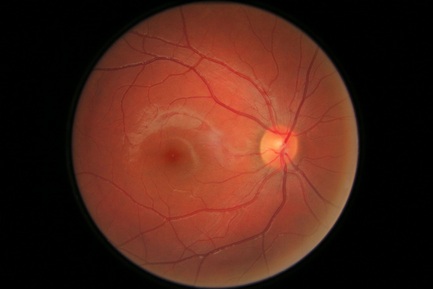 An image of my own Retina: Right eye |
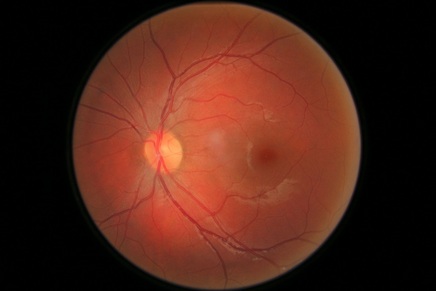 An image of my own Retina: Left eye |
The above images show a normal Retina, both of the right and left eye. There are no signs of Diabetic Retinopathy.
Diabetic Retinopathy
Risk factors
Classification of Diabetic Retinopathy
Non-proliferative Diabetic retinopathy, also called background diabetic retinopathy
This is characterised by microaneurysms, ‘dot and blot’ haemorrhages, hard yellow exudates.
Pre-proliferative retinopathy
This is an intermediate stage between ‘background’ and proliferative retinopathy and consists of increasing signs of retinal ischaemia.
- Duration of diabetes – This increases the prevalence of retinopathy drastically.
- Control of diabetes – glycaemic control is important as it lessens the risk of retinopathy in both type 1 and type 2 diabetics.
- Hypertension – Tight control of blood pressure reduces the risk of complications related to diabetes and also death related to diabetes. (<140mmHg systolic and <85mmHg diastolic). The United Kingdom Prospective Diabetes Study (UKPDS) found that good control of blood pressure reduced the risk of diabetic retinopathy.
- Hyperlipidaemia – This is a risk factor which is more important in type 2 diabetics who are at an increased risk of developing macular oedema.
- Nephropathy – If this is severe, this can be associated with worsening of retinopathy and maculopathy. It is partly related to hypertensive and lipoprotein abnormalities.
- Pregnancy – This can accelerate the rate development and progression of diabetic retinopathy.
- Cataract – Cataract development is common in diabetics. This is also important as cataract surgery in diabetic patients can worsen maculopathy and proliferative retinopathy.
- Late presentation – Patients who present to screening clinics late have a much worse prognosis visually, than if the retinopathy was diagnosed earlier.
- Others – smoking, obesity, hypercholesterolaemia,
Classification of Diabetic Retinopathy
Non-proliferative Diabetic retinopathy, also called background diabetic retinopathy
This is characterised by microaneurysms, ‘dot and blot’ haemorrhages, hard yellow exudates.
- Microaneurysms – These are the earliest changes which occur and appear as dilated retinal veins and capillaries. The excess glucose in diabetes causes the shunting of glucose into the aldose reductase pathway resulting in the formation of Sorbitol. Sorbitol can affect the intramural pericytes in the retinal blood vessels causing them to lose their autoregulatory function. This causes outpouching of the capillary walls.
- ‘Dot and blot’ haemorrages -The microaneurysms can rupture resulting in leakage of blood. Superficial haemorrhages appear as ‘flame-shaped’ whereas haemorrhages in deep layers of the retina appear as ‘dots and blots’.
- Hard yellow exudates - extracellular accumulations of protein and lipid as serum leaks through the abnormal blood vessel walls.
Pre-proliferative retinopathy
This is an intermediate stage between ‘background’ and proliferative retinopathy and consists of increasing signs of retinal ischaemia.
- Cotton wool spots - damage to nerve fibres as a result of swelling on the surface layer of the retina due to infarction.
- Venous beading - due to retinal ischaemia
- Sausage-shaped dilatations of retinal veins, venous loops and reduplication of the vessels occur due to retinal ischaemia
- IRMA – Intraretinal Microvascular Abnormalities - abnormal-looking and dilated veins in areas of non-perfused retina.
The early treatment diabetic retinopathy study [ETDRS] found that multiple retinal haemorrhages, changes in venous calibre and IRMA are signs which indicate a risk of progression to proliferative diabetic retinopathy.
Proliferative retinopathy
Proliferative retinopathy
- This involves the growth of new blood vessels in the retina, called Neovascularisation. This occurs due to retinal hypoxia, as blood vessels close-off, which triggers the release of vasoproliferative factors. New vessels can also arise on the iris, which is called Rubeosis Iridis.
- Proliferative Diabetic Retinopathy is divided into two categories. Vessels which are located within one disc diameter from the optic disc are called Neovascularisation of the disc (NVD). Vessels located greater than this diameter from the optic disc are called Neovascularisation elsewhere (NVE).
- New vessels grow well on connective tissue framework, such as the posterior vitreous face which is partially detached. Traction on these vessels can cause vitreous haemorrhage which can reduce vision.
- Tractional retinal detachment – This can be caused by fibro-vascular proliferation.
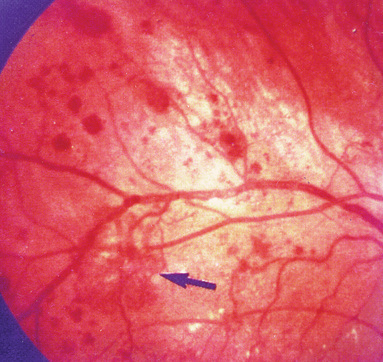
Neovascularisation Elsewhere (NVE)
Taken From: K. Viswanath et al.
J. Comm. Eye Health 2003;16(46) 22
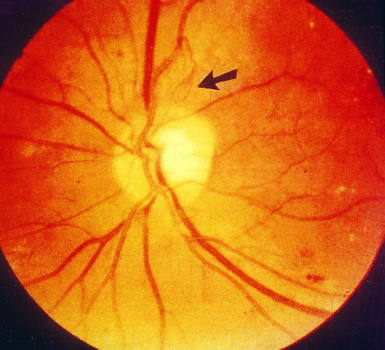
Neovascularisation of the Disk (NVD)
Taken from: K. Viswanath et al.
J. Comm. Eye Health 2003;16(46) 22
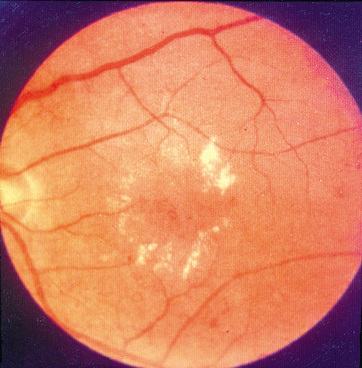
Diabetic Maculopathy
Diabetic Maculopathy affects the macula and is therefore a leading cause of blindness in non-proliferative diabetic retinopathy patients. It is further divided into different types.
Macular oedema is thought to be caused by a breakdown of the blood-retinal barrier.
Diabetic Maculopathy affects the macula and is therefore a leading cause of blindness in non-proliferative diabetic retinopathy patients. It is further divided into different types.
- Focal macular oedema – This arises from microaneurysms, where fluid leaks into the retina. It is usually seen with well-circumscribed rings of hard exudates which consist of lipid and lipoprotein material that has precipitated.
- Diffuse macular oedema – This arises from large areas of damaged capillaries, microaneurysms and capillary beds of dilated vessels. This can also occur with cystoid macular oedema.
- Clinically Significant Macular Oedema (CSMO) – This is when there is retinal oedema within 500µm of the centre of the fovea. There are also hard exudates and retinal thickening.
- Ischaemic maculopathy – The perifoveal capillaries close-off reducing perfusion in the macula.
Macular oedema is thought to be caused by a breakdown of the blood-retinal barrier.
Diabetic Maculopathy
Taken From: K. Viswanath et al.
J. Comm. Eye Health 2003;16(46) 22
Other complications of Diabetes
Lids and Orbit
- Orbital Cellulitis – Mucormyces mucor is an anaerobic fungus, which is a commensal in most individuals. In diabetic patients with immunoparesis, it can cause a life-threatening infection. It can invade endothelial cells and cause necrotising vasculitis. A black eschar appears on the eyelids or palate.
Cornea
- Neurotrophic keratopathy – The trigeminal nerve can be affected in long-standing diabetes. Since the trigeminal nerve supplies corneal sensation, this can be affected and can predispose patients to recurrent infections.
- Infectious keratitis – This may occur due to a neurotrophic cornea. It can also occur because of microtrauma.
- Fungal keratitis – Diabetic patients are predisposed to fungal keratitis, mainly with Candida spp. Symptoms which occur are a painful eye, conjunctival injection and a white corneal infiltrate.
Lens
- Refractive instability – osmotic changes, due to changes in glucose levels, can cause the lens to swell. This can cause blurring of vision.
- Cataract - true diabetic cataract (rare), senile cataract in diabetic (common). There can be sudden changes in refraction – especially when diabetes is not controlled.
Pupil responses
- Diminished pupillary responses – due to glycogen infiltration of the pigment epithelium.
Back to top
