Thyroid disease and the eye
Hyperthyroidism
Hyperthyroidism is a hypermetabolic disorder which is associated with the overproduction of Free thyroxine (FT4) and/or free triiodothyronine (FT3). Its systemic complications involve a goitre, fine hand tremor, intolerance to warmth, weight loss, diarrhoea, vitiligo, tachycardia and acropachy (clubbing of fingernails).
Graves Disease
Graves disease is an autoimmune disease which involves the thyroid gland and orbital tissues. It is the most common cause of hyperthyroidism. Antibodies for the anti-TSH receptor cause an increased production of Thyroxine (T4) and T3. The complications arise from the immune cells attacking the thyroid and ocular tissue. Most patients with Graves disease have an overactive thyroid but patients with normal thyroid function can also have Graves Disease. Women are more likely to be affected than men. However, when men are affected it tends to be more severe.
Pathogenesis of eye disease:
The cause is still unclear. However, it is likely that the target antigen for the retro-orbital tissues and the thyroid gland are the same. This could cause activated T cells to act on cells in the orbit, stimulating adipogenesis, fibroblast proliferation and glycosaminoglycan synthesis. The extraocular muscles and retro-ocular connective tissue become infiltrated by lymphocytes causing an activation of cytokines and inflammation. The volume of the extraocular muscles, retro-orbital fat and connective tissue increases.
Lids
- Periorbital puffiness and swelling
- Lid lag – on downgaze, called Von Graefe’s sign.
- Lid retraction – upper lid is usually more retracted than the lower lid. This is due to excessive stimulation of the sympathetically innervated muscles of the eyelids. This also causes lid lag. Restrictive myopathy of the inferior rectus muscle can also cause lid retraction as there is increased stimulation of the levator muscle on upgaze.
Lacrimal system
- Excessive lacrimation
Conjunctiva/sclera
- Staining - as a result of exposure
- Gritty red eyes
- Chemosis – conjunctival oedema
- Increased vascularity – near the insertion of the extraocular muscles
- Superior limbic keratoconjunctivitis - inflammation of the superior bulbar conjunctiva. The superior limbus is predominantly involved.
Cornea
- Exposure – caused by excessive proptosis and lid retraction. Also restriction of the inferior recti with loss of Bell’s Phenomena (an upward and outward movement of the eye when an attempt is made to close the eye).
- Proptosis – Protusion of the eyes anterior displacement of the globe by enlarged oedematous extraocular muscles and orbital fat. This causes exopthalmos and lid retraction.
- Ulceration – can occur due to sever exposure.
Optic nerve
- Compression – caused by the enlargement of the extraocular muscles on the apical portion of the optic nerve. This can increase intraocular pressure.
- Optic neuropathy – This is quite rare. There can be swelling of the head of the optic nerve. There may also be choroidal folds as a result of pressure on the globe.
Eye movements
- Restriction of eye movements – infiltration of inflammatory cells within the muscles. This can cause more inflammation, oedema and fibrosis. Diplopia and strabismus can occur also.
Other complications:
- Diplopia (double vision)
- Rise in intraocular pressure which sometimes worsens on upward elevation of the eye.
Taken from: Perros et al. BMJ 2009; 338:b560
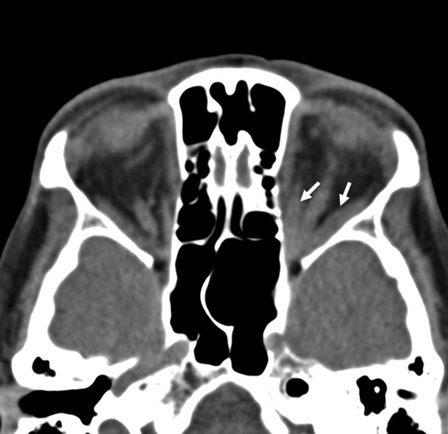
CT Scan of Thyroid orbitopathy. The Medial and inferior rectus muscles are thickened (shown by arrows)
Taken from: Perros et al. BMJ. 2009; 338:b560
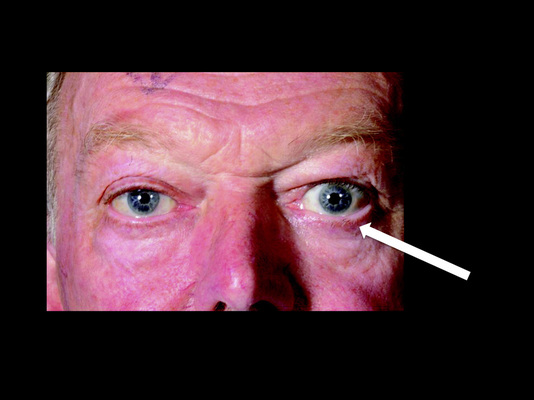
Patient with mild Exopthalmos in the left eye (indicated by arrow)
The above images have been used with permission from Dr Petros Perros.
